Does anyone have any evidence (3 rings facial colouration) that this works?
Not yet verified -this observation came from the real 'front line' and is only 24 hours or so old.

Does anyone have any evidence (3 rings facial colouration) that this works?
Not yet verified -this observation came from the real 'front line' and is only 24 hours or so old.
Alan Smith Thanks.

So Trump is going ahead with chloroquine testing - great news.
Not just testing, but making it available.
https://www.foxnews.com/politi…imental-drugs-coronavirus
While the trial is still out, it seems enough support to make this credible. Give credit where due.... Dr. Richard may have been prophetic on this one!
However, you can be sure, if Trump is behind it... it is idiotic and should not be done! ![]() (Sorry could not resist.)
(Sorry could not resist.)
From: https://www.nbcnews.com/health…ting-coronavirus-n1158316
QuotePreliminarily, it seems at least two hospitalized patients who received remdesivir started to feel better the next day.
Infuriating. Meaningless. How would you know they were not getting better anyway. And how is feeling better a criterion? It's entirely subjective. How about measurements? Fever, virus assays, blood counts, CT scans, etc. ? That's why you need a research series, a control group, randomized selection and patient matching between groups. Nor does doing it right, especially in a preliminary study, take all that long as evidenced by the hydroxychloroquine and azithromycin study from France posted earlier. They didn't meet all desired research criteria but they did meet the minimum one: a control group of untreated individuals for comparison to the treated group. Oh, and objective criteria for improvement (viral counts).
Geez! The general ignorance of scientific method among the general public and particularly certain reporters, is staggering!

And here are a couple of accounts on the use of remdesivir:
That's exactly what the pharma mafia hopes 10000$ investors blow job /dose! Instead of 2 generics (Azithromycin, hydroxychloroquine? (Plaquenil) that work fine if combined.
QuoteWhile the trial is still out, it seems enough support to make this credible. Give credit where due.... Dr. Richard may have been prophetic on this one!
No he or she wasn't. Throwing in everything but the kitchen sink and having one prediction work out isn't being prophetic any more than a psychic cold reading you is.
QuoteHowever, you can be sure, if Trump is behind it... it is idiotic and should not be done!
Where to start with that? On this forum? In this instance, Trump is simply repeating what some of his experts have told him.
Wyttenbach FACEPALM!
Display MoreSorry if this was posted before, it's hard to keep up. It's about some very preliminary but promising, controlled (more or less) trials of hydroxychloroquine and azythromycin in reducing viral load in human patients who had COVID-19 infections.
Expect a PDF download or display depending on how your system is setup. I tried it and no malware warnings.
https://www.mediterranee-infec…oquine_final_DOI_IJAA.pdf
I have not read the details yet. I do know from the TV interview I saw that it was not a blinded study nor was it randomized. It is a very small series of appx 20 subjects who got the drugs and 20 who did not. The control subjects were in no way matched with the experimental subjects so please: THIS IS A VERY WEAK STUDY. Nonetheless, if it is borne out, it is very exciting. Both hydroxychloroquine (or chloroquine) and azithromycin should be cheap and readily available in large quantities. And they are relatively safe, Certainly safer than having a significant infection with COVID-19. And it should not take too long to replicate in a much more "rigorous" fashion. So promising (all patients receiving the drug went to zero virus levels) but weakly controlled and:
- not matched subjects
- not randomly split between controls and experimental group
- not blinded
- very small "series" (groups)
So be optimistic but also be skeptical.
It is interesting as a study. The lack of random patient selection is worrying: much more so if we reckon unconscious biasses on part of experimenter could determine this.
The methodology is also questionable.
We enrolled 36 out of 42 patients meeting the inclusion criteria in this study that had at least
six days of follow-up at the time of the present analysis. A total of 26 patients received
hydroxychloroquine and 16 were control patients. Six hydroxychloroquine-treated patients
were lost in follow-up during the survey because of early cessation of treatment. Reasons are
as follows: three patients were transferred to intensive care unit, including one transferred on
day2 post-inclusion who was PCR-positive on day1, one transferred on day3 post-inclusion
who was PCR-positive on days1-2 and one transferred on day4 post-inclusion who was PCRpositive
on day1 and day3; one patient died on day3 post inclusion and was PCR-negative on
day2; one patient decided to leave the hospital on day3 post-inclusion and was PCR-negative
on days1-2; finally, one patient stopped the treatment on day3 post-inclusion because of nausea
and was PCR-positive on days1-2-3. The results presented here are therefore those of 36
patients (20 hydroxychloroquine-treated patients and 16 control patients). None of the control
patients was lost in follow-up
The question is are the "lost" patients consistently biased in terms of expected outcomes.
1 died, after being PCR-negative for 1 day
3 were transferred to ICU after being PCR-positive
2 chose to stop treatment (one of whom had been PCR-negative days 1-2, 1 PCR-positive with nausea)
There is bias here, but it is not clearly one way or the other, and not enough to make results uninteresting.
Also, the active group is all from the Marseilles center, the control group mostly from other centers, with an unstated number who refused treatment from Marseille. There is at least one difference in protocol:
control patients from centers other than Marseille did not underwent daily sampling, but were sampled every other day in most cases, they were
considered positive for PCR when actually positive the day(s) before and the day(s) after the day(s) with missing data.
this difference (the AND) means that controls are more likely to be counted negative than actives, so this actually strengthens the results.
So:
It is a very weak study
Cannot rule out bias that would entirely explain the results
If no bias it is highly interesting
Let us hope we get a lot more testing of this.
THH
From: https://www.nbcnews.com/health…ting-coronavirus-n1158316
Infuriating. Meaningless. How would you know they were not getting better anyway. And how is feeling better a criterion? It's entirely subjective. How about measurements? Fever, virus assays, blood counts, CT scans, etc. ? That's why you need a research series, a control group, randomized selection and patient matching between groups. Nor does doing it right, especially in a preliminary study, take all that long as evidenced by the hydroxychloroquine and azithromycin study from France posted earlier. They didn't meet all desired research criteria but they did meet the minimum one: a control group of untreated individuals for comparison to the treated group. Oh, and objective criteria for improvement (viral counts).
Geez! The general ignorance of scientific method among the general public and particularly certain reporters, is staggering!
yeah they do acknowledge in the article that the two people who used remdesivir may have just gotten better on their own without the drug. Remdesivir is in clinical trials now and results aren’t in until April. So they are in a silent period. We simply will have no idea if it works at all until the first results are published in April.
remdesivir is an interesting drug though. It’s sole purpose is to stop viruses from replicating. It was developed to treat Ebola, but it didn’t work.
Trump may be encouraging the FDA to work a little bit faster..
"U.S. FDA Commissioner Stephen Hahn addressed the ongoing work of the agency in terms of its work on potential treatments and vaccines for the COVID-19 coronavirus currently spreading globally.
Despite a claim early in Thursday’s White House briefing on the pandemic by President Donald Trump that one proposed treatment, anti-malarial chloroquine,
had already been approved by the FDA for COVID-19 treatment,
Hahn said that in fact the agency is currently looking at widespread clinical trials of the drug, but it is not yet approved for that use."
https://techcrunch.com/2020/03…overed-covid-19-patients/
3:45 am AEDT • March 20, 2020
https://www.newsmax.com/health…rus/2020/03/19/id/959061/
Bayer Donates 3M Malaria Tablets to US Coronavirus Fight
Read Newsmax: Bayer Donates 3 Mln Malaria Tablets to U.S. for Potential Use against Coronavirus | Newsmax.com
Hopefully the Chinese data and the FDA data show its effective
Its cheap,
Chloroquine was discovered in 1934 by Hans Andersag.[4][5]
It is on the World Health Organization's List of Essential Medicines, the safest and most effective medicines needed in a health system.[6]
It is available as a generic medication.[1]
The wholesale cost in the developing world is about US$0.04.[7] In the United States, it costs about US$5.30 per dose.[1]
O dragging their feet now but good news from Bayer! Do they read our eccentric forum? They donated a similar smaller quantity to rescue China in February which "unofficially' brought their epidemic under contrpl. All infected patients across the planet should be given the option of this antiviral therapy. This is not prophecy it's just simple investigative bioscience which I am an trained in having a doctorate in Biophysics (like Piantelli!).
HANDLING CORONAVIRUHow to respond to COVID-19
And prepare for the next epidemic, too.
Bill Gates donated 100 Million to the Covid cause..and had a Q/a on reddit recently
https://www.gatesnotes.com/Health/How-to-respond-to-COVID-19
https://www.reddit.com/r/Coron…f_the_bill_melinda_gates/
Grab your tonic water from Tescos before it sells out like loo roll - check other brands for quinine hydrochloride rather than quinine flavoring. Add![]() some gin and have a party to celebrate the end of COVID-19!
some gin and have a party to celebrate the end of COVID-19!
Working from home? Which one?
It has occurred to me that if I lived in a country where I thought the health service was likely to get swamped and disfunctional with the number of cases in a few weeks then maybe the logical thing to do is to make sure that I would catch the Corona virus now while there is access to the best care.
Not a great choice to have to consider and hopefully in the UK not a likely scenario.
Working from home? Which one?
must be from his doomsday yatch.
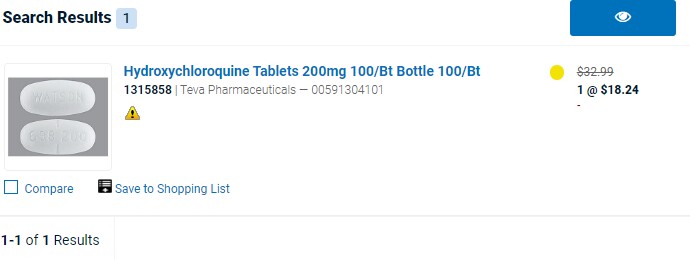
QuoteIn the United States, it costs about US$5.30 per dose.
Really? Here is the cost from a medical supply house (Schein Medical)
So the triangle with the exclamation point means you have to have a medical license to buy it from these guys (or appropriate institutional credentials). The yellow dot means "currently on back order" and they do not say when shipments are expected but this company is usually pretty prompt.
Retail pharmacy price in the US is around $20 for 60 tablets. YMMV and of course, depends on location.
https://www.goodrx.com/coupon?…macy_id=31240&quantity=60
Note that the optimal dose, if it even actually works, is not determined yet but possibly could be between 200 and 600 mg once or twice a day for a week. The drug is very long lasting in blood and tissues.
Grab your tonic water from Tescos before it sells out
Funnily enough I was there today - all the cheap brands sold out- but I bought 'Fever Tree' which does have some smidgins of real quinine in. This btw was a superstore, but it has many empty shelves. They have around 50 meters of cold cabinets of fresh meat (normally) - today all of them were completely empty. Not even any horsemeat.