https://corporate.dukehealth.o…lp-relieve-shortages?h=nl
Strong hydrogen peroxide "vapor" can decontaminate N95 masks for reuse.

https://corporate.dukehealth.o…lp-relieve-shortages?h=nl
Strong hydrogen peroxide "vapor" can decontaminate N95 masks for reuse.

JedRothwellis precisely correct on the above. The only thing that will end the crisis in the US and the developed world is a fast test, preferably done without a machine like a pregnancy test. Then, meticulous case tracing and quarantining positive cases. We will probably also know from immunoglobulin studies who has sufficient immunity.
This is what Fauci said the other day. It is what the Japanese and Koreans have been telling us for weeks. Today, the New York Times editorial board finally got the message:
How American Can Reopen
A very good structural and genomic analysis of Cov-2 compated to CoV-1, others and some other joyfulness ahead.
https://www.youtube.com/watch?v=8_bOhZd6ieM&t=1224s
Here are my notes, from what I understood.... this is highly technical so thanks for your understanding :
20200402
Quotes and notes from the video, everything within parenteses is from the autor:
Conclusion on what is new:
Best
Thank you Mathieu.
A couple of very recent papers propose soluble angiotensin-converting enzyme 2 as a promising therapy --
"Inhibition of SARS-CoV-2 infections in engineered human tissues using clinical-grade soluble human ACE2"
Summary
We have previously provided the first genetic evidence that Angiotensin converting enzyme 2
(ACE2) is the critical receptor for SARS-CoV and that ACE2 protects the lung from injury,
providing a molecular explanation for the severe lung failure and death due to SARS-CoV
infections. ACE2 has now also been identified as a key receptor for SARS-CoV-2 infections and
it has been proposed that inhibiting this interaction might be used in treating patients with COVID19.
However, it is not known whether human recombinant soluble ACE2 (hrsACE2) blocks growth
of SARS-CoV-2. Here we show that clinical grade hrsACE2 reduced SARS-CoV-2 recovery from
Vero cells by a factor of 1,000-5,000. An equivalent mouse rsACE2 had no effect. We also show
that SARS-CoV-2 can directly infect engineered human blood vessel organoids and human kidney
organoids, which can be inhibited by hrsACE2. These data demonstrate that hrsACE2 can
significantly block early stages of SARS-CoV-2 infections.
https://www.cell.com/pb-assets…/CELL_CELL-D-20-00739.pdf
"Soluble angiotensin-converting enzyme 2: a potential approach for coronavirus infection therapy?"
Abstract
A new coronavirus, referred to as SARS-CoV-2, is responsible for the recent outbreak of severe respiratory disease. This outbreak first detected in Wuhan, China in December 2019, has spread to other regions of China and to 25 other countries as of January, 2020. It has been known since the 2003 SARS epidemic that the receptor critical for SARS-CoV entry into host cells is the angiotensin-converting enzyme 2 (ACE2). The S1 domain of the spike protein of SARS-CoV attaches the virus to its cellular receptor ACE2 on the host cells. We thought that it is timely to explain the connection between the SARS-CoV, SARS-CoV-2, ACE2 and the rationale for soluble ACE2 as a potential therapy.
https://portlandpress.com/clin…sin-converting-enzyme-2-a
However, if I have properly identified the above enzyme with this available lab enzyme --
https://www.sigmaaldrich.com/c…/176872?lang=en®ion=US
-- the cost may be prohibitive
Regarding the presentation above, one of the items sticks out to me:
“The spike protein is an identical mean of penetration into the cell membrane we can find for Ebola and HIV viral infections.”
I think there was some surprise within the medical community about why antivirals for HIV haven’t been more effective against Covid in studies. If the virus is penetrating the cell in the same way, it’s understandable that they went to those drugs first. But they haven’t been shown to work. They are still trying, but the logic is there for antivirals for HIV having some level of effectiveness against it.
Here are some interesting studies being launched by WHO:
https://news.yahoo.com/coronav…ornia-herd-103032367.html
Interesting explanation as to why California so far has seen very little COVID activity. Speculation as they readily admit, but the theory is that the early fall "severe flu" they experienced, was in fact COVID. As a result, California residents developed Herd Immunity, which has made conditions tough for the virus to gain a foothold.
https://www.medrxiv.org/conten…101/2020.03.11.20031096v2
QuoteAbstract
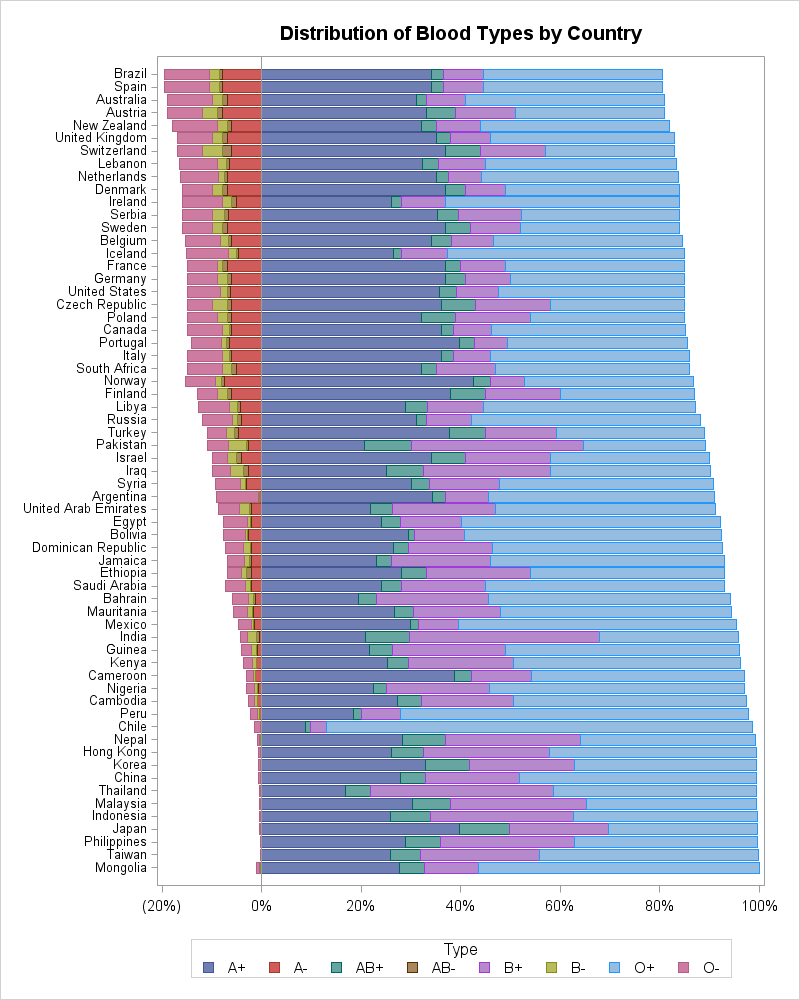
The novel coronavirus disease-2019 (COVID-19) has been spreading around the world rapidly and declared as a pandemic by WHO. Here, we compared the ABO blood group distribution in 2,173 patients with COVID-19 confirmed by SARS-CoV-2 test from three hospitals in Wuhan and Shenzhen, China with that in normal people from the corresponding regions. The results showed that blood group A was associated with a higher risk for acquiring COVID-19 compared with non-A blood groups, whereas blood group O was associated with a lower risk for the infection compared with non-O blood groups.
https://figshare.com/articles/…id-19_infections/12019035
How blood group A might be a risk and blood group O be protected from coronavirus (COVID-19) infections
Preprint posted on 02.04.2020, 06:38 by Peter Arend
QuoteIn the case that O-glycosylation plays a key role in the pathogenesis of coronavirus infections, as was discussed already 14 years ago and is currently again predicted, this would result in the formation of a serologically A-like, O-GalNAcα1-Ser/Thr-R, Tn (“T nouvelle”) antigenic structure; the virus hypothetically hijacks the metabolism of the host's amino sugar N-acetyl-D-galactosamine (GalNAc) by serine-rich peptides. This intermediate, evolutionary/developmental A-like/Tn structure, which is common to all metazoan growth processes and apparently acts as a host-pathogen functional bridge in different, unrelated infectious diseases, would perform the adhesion of the virus to host cells primarily independent of the ABO blood group. However, while susceptibility to an infection and its severity depend on many factors, individuals with blood group A could not respond with either acquired or innate antibodies to the synthesis of A-like hybrid structures due to clonal selection and phenotypic accommodation of plasma proteins; they would become a preferred target for the virus, which utilizes the A-phenotype-determining glycotransferase, performing a further (blood group-A-specific) hybrid binding. In fact, a first statistical study suggests that people with blood group A have a significantly higher risk for acquiring COVID-19, whereas people with blood group O have a significantly lower risk for the infection compared with non-O blood groups (Zhao, J. et al., 2020). While these findings await confirmations, blood group O individuals, lacking the blood group-A-determining enzyme, would develop the least molecular contact with the virus and maintain the anti-A/Tn cross-reactive, complement-dependent isoagglutinin activity, which is exerted by the polyreactive, nonimmune immunoglobulin M (IgM), representing the humoral spearhead of innate immunity and a first line of defense.

blood group A might be a risk and blood group O be protected
but what about me. I am type B.
The use of a ventilator in the treatment of acute COVID is a prime factor in the determination of the lethality of that condition. It is possible to model the impact on lack of availability of ventilators as a function of the total death count.
If a patient admitted into treatment with pneumonia when a ventilators is not available for his treatment, the chance of his death in that patient is 50%. The assumption in the modeling now assumes that ventorators will always be available to produce a ideal minimum death count of 240,000. If ventilators are maxed out close to current levels, then the death count will most likely exceed a probable death count in the high hundreds thousands or more.
It is entirely possible in modeling this maximum death count, to project that count against the production plans for ventilators.
If the availability of ventilators in the marketplace is used to maximize profits for their sale, then the death count could reach a million or more.
It appears to be a direct tradeoff condition between ventilator profit margins and death count at play here.
QuoteInteresting explanation as to why California so far has seen very little COVID activity. Speculation as they readily admit, but the theory is that the early fall "severe flu" they experienced, was in fact COVID. As a result, California residents developed Herd Immunity, which has made conditions tough for the virus to gain a foothold.
Baseless and useless speculation. It is possible to test for COVID-19 immunoglobulin antibodies. If this idea is of interest, do the tests and STFU until you have the evidence (not you, Shane, the authors of whatever you read or heard). The tests are still a research only activity but hopefully soon, it will be possible to test everyone for possible immunity to COVID-19.
Baseless and useless speculation. It is possible to test for COVID-19 immunoglobulin antibodies.
Nothing wrong with speculation to start the discussion off. We do it here on the forum all the time. It is interesting that California, with a population of 40,000,000, only has 11,000 confirmed cases. Why? They only started isolation 11-12 days ago, so doubtful that has made them an outlier in the US. They do have a large Chinese population, resulting in busy two-way travel with China, which should have made them as vulnerable as New York.
The antibodies could determine if the Herd Immunity speculation is true, and those test kits are becoming widely available. No doubt there will be a follow up study.
https://www.washingtontimes.co…ost-effective-therapy-do/
Doctors do not like to speak on the record, but poll them anonymously, and they will tell you what they think. Worldwide, according to this poll, Doctors use HCQ as their #1 treatment for COVID. This is the kind of pressure that will help break down those bureaucratic barriers preventing free usage.

Herd Immunity
Maybe there is less herd in LA
LA noncondensed 'chill' versus NY close 'hustle' might be a factor.
QuoteIt is interesting that California, with a population of 40,000,000, only has 11,000 confirmed cases. Why?
It's because they are still low on the infection rate curve. Probably because the virus was introduced later than elsewhere or more slowly. Sure, it's worth knowing if it's due to immunity but that is very extremely improbable. And sadly, the number of cases will grow a lot in California because, as we see on the TV and on the streets every day, there are plenty of knuckleheads who don't "believe in it" or don't take it seriously or are too dumb to follow instructions.

Maybe there is less herd in LA
LA noncondensed 'chill' versus NY close 'hustle' might be a factor.
External Content www.youtube.comContent embedded from external sources will not be displayed without your consent.Through the activation of external content, you agree that personal data may be transferred to third party platforms. We have provided more information on this in our privacy policy.
Yes, good point. NYC is not only more tightly packed than the big 3 Ca cities (SF, LA, SD.), but their residents habits bring them in much closer contact for almost every daily lifestyle activity they do. Not sure that would explain away such a large discrepancy though.
It's because they are still low on the infection rate curve. Probably because the virus was introduced later than elsewhere or more slowly. Sure, it's worth knowing if it's due to immunity but that is very extremely improbable. And sadly, the number of cases will grow a lot in California because, as we see on the TV and on the streets every day, there are plenty of knuckleheads who don't "believe in it" or don't take it seriously or are too dumb to follow instructions.
I find it implausible that California "was introduced later than elsewhere. or more slowly"...to the virus. The article makes a strong case that is not true. They claim just the opposite in fact... that it was introduced in California, and *early*, as in the fall. Even before China "officially" recorded their first case on Dec 1st I think it was.
And what do you mean "or more slowly"? How would a virus be introduced more slowly?
I find it implausible that California "was introduced later than elsewhere. or more slowly"...to the virus. The article makes a strong case that is not true. They claim just the opposite in fact... that it was introduced in California, and *early*, as in the fall. Even before China "officially" recorded their first case on Dec 1st I think it was.
And what do you mean "or more slowly"? How would a virus be introduced more slowly?
If this is the case,
Then the flu did NOT originate in China?