
We in the UK are definitely the 'control' group in Europe with case numbers and daily death numbers remaining stable over the last three weeks whereas Italy, Spain and Germany whose doctors are now routinely prescribing HCQ and Avigan are showing definite falls over the same period. This is depressing.

Dr Richard
Verified User
- Member since Sep 19th 2018
- Last Activity:
Posts by Dr Richard
-
-
Psilocybin is pretty good too in magic mushrooms - Prof Nutt at Imperial has been recommending it for depression for years. Nothing like speed and coke to lift the mood as Ozzy from Sabbath used to say in between biting off bat's heads. Maybe that's what started this outbreak......

-
Yes they are hoping the problem will just disappear as suddenly as it arrived - because that's what happened in previous SARS and MERS outbreaks. It will all be over when summer comes! What else do you expect from politicians?
-
Standard practice tends to be thrown out of the window when things become this desperate. We end up with using anything that has a chance of being effective to save lives. More in vitro tests of other CQ analogues, doxycycline instead of azithromycin finding the best treatment options takes time and money, animal experiments are needed too for preliminary in vivo studies as oldguy has suggested. Our so-called advanced Western medical system has been caught napping by this coronavirus outbreak with all our advances in molecular biology, gene mapping, RNA virus vaccines, antibody screening etc we were arrogantly confident about handling this before it hit us this hard. Hence the initial government inaction in delaying quarantine measures and it's the hubris within the medical profession that is delaying roll out of potential treatments especially in the UK.
-
Top 15 Foods High in Zinc and Their Health Benefits - Dr. Axe
draxe.com › Nutrition › Vitamins & Minerals
30 Apr 2019 - Reports suggest that people who don't eat meat or animal products, like people on a vegetarian or vegan diet, need up to 50 percent more zinc ..Well even consuming 100g of prime steak only gives you 4.8 mg Zn - so the 220 mg dose is probably appropriate in boosting HCQ effectiveness. Running up to toxic levels though, so may have to give some iron to counter Zn toxicity.
-
More maps of Costa Rica again malaria areas have v low COVID-19 cases
Map of provinces with confirmed coronavirus cases (as of 15 April) Confirmed 1–9 Confirmed 10–99 Confirmed 100–315
Map of cantons with confirmed coronavirus cases (as of 15 April) Confirmed 1–9 Confirmed 10–82 Disease Malaria map
meat diets
Most meat/fish diets will supply sufficient Zn, only need extra if deficiency is suspected as in the veteran's case - or if on a vegan diet perhaps?
-
So Costa Rica is effectively adopting Mass Fever Treatment with hydroxychloroquine but not the less targeted Mass Drug Adminitration approach. Good for them, hope the WHO will recommend this soon to limit the pandemic worldwide.
-
Costa Rica has a far more progressive attitude and is successfully treating the pandemic. Unrestrained by EU US WHO thinking. Makes me ashamed that the UK is so backward.
“We are not adopting a protocol from another country just for the sake of it. We are responsible and we verify that what they present is true and convincing. Their experience is valid. The studies published are international, but on the other side, we have a life-threatening infection.
“Therefore, it is necessary to approach the patient with decisions based on the best scientific evidence that exists in a situation such as the current one in order to make a public health decision,” Obando said.
Avoid the ICU at all costs
Hydroxychloroquine and chloroquine are “first cousins,” explained Olga Arguedas, who is a specialist in immunology. Both drugs have chemical compositions and medical uses that are not exactly the same.
“They are old acquaintances. They are registered in Costa Rica and are produced locally. This was taken into account as an important point in the decision to give hydroxychloroquine as treatment. They are known because they have antiviral mechanisms. Hydroxychloroquine was used in Shanghai as the first line of treatment,” said Arguedas.
The specialist in immunology explained the drug has been used in Brazil and France and the Revista Panamericana de Salud Pública summarized all the treatments that are being published for covid-19. Those in more advanced stages (with more scientific information) are those where hydroxychloroquine has been used.
“We still cannot be sure because there is no scientific evidence. However, in the very particular case of Costa Rica, this could be one of the elements that is influencing the good results of the country so far,” added Arguedas.
She emphasized that the purpose pursued with the use of hydroxychloroquine is to mitigate the progression of the disease.
-
Doxycycline instead of Azithromycin maybe? A cardioprotective antibiotic also used as an anti malarial:
Doxycycline to Protect Heart Muscle After Heart Attacks - Full ...
clinicaltrials.gov › show › NCT03508232
25 Apr 2018 - The participants in this study showed no adverse effects of using ... Doxycycline decreases intracellular proteolysis, improves cardiac function, ... -
Because of recent declining malaria transmission in Latin America, some authorities have recommended against chemoprophylaxis for most travelers to this region. However, the predominant parasite species in Latin America, Plasmodium vivax, can form hypnozoites sequestered in the liver, causing malaria relapses. Additionally, new evidence shows the potential severity of vivax infections, warranting continued consideration of prophylaxis for travel to Latin America. Individualized travel risk assessments are recommended and should consider travel locations, type, length, and season, as well as probability of itinerary changes. Travel recommendations might include no precautions, mosquito avoidance only, or mosquito avoidance and chemoprophylaxis. There are a range of good options for chemoprophylaxis in Latin America, including atovaquone-proguanil, doxycycline, mefloquine, and—in selected areas—chloroquine. Primaquine should be strongly considered for nonpregnant, G6PD-nondeficient patients traveling to vivax-endemic areas of Latin America, and it has the added benefit of being the only drug to protect against malaria relapses.
All these anti-malarial drugs have been restricted since the coronavirus outbreak - urgent testing of all CQ analogues in use today should be done against COVID-19. Or just ask Elon Musk for his opinion after surviving a dose of malaria.
-
Still, given the choice of taking anti-malaria medicine on developing fever surely most people would take it given the option? That is the point whether outbreaks of malaria are recent or not probably doesn't matter-its the cultural memory of having had a dose of malaria - the symptoms could not be distinguished from early symptoms of COVID-19. The Government response obviously is also important in limiting the spread.
-
Malaria/COVID-19 maps update from wiki:
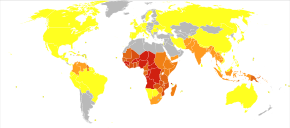
Deaths due to malaria per million persons in 2012 0–0
1–2
3–54
55–325
326–679
680–949
950–1,358
Past and current malaria prevalence in 2009
Map of confirmed cases of COVID-19 per capita (as of 23 April 2020): > 2000 cases per million inhabitants
500–2000 cases per million inhabitants
200–500 cases per million inhabitants
50–200 cases per million inhabitants
>0–50 cases per million inhabitants
No reported cases, no population, or no data available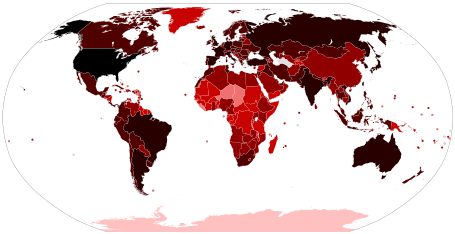
Total confirmed cases of COVID-19 by country and territory (as of 23 April 2020): 100,000+ confirmed cases
10,000–99,999 confirmed cases
1,000–9,999 confirmed cases
100–999 confirmed cases
10–99 confirmed cases
1–9 confirmed cases
No confirmed cases or no data
Total confirmed deaths per million of COVID-19 by country and territory (as of 23 April 2020): 100+ deaths per million inhabitants
10–100 deaths per million inhabitants
1–10 deaths per million inhabitants
0.1–1 deaths per million inhabitants
0.01–0.1 deaths per million inhabitants
No deaths or no dataThis article provides a general overview and documents the status of locations by continents and conveyance of the world affected by the coronavirus responsible for the ongoing 2019–20 pandemic originating in Wuhan, Hubei, China. It may not include all the most up-to-date major responses and measures by individual countries and territories.
-
Same applies to the only EU country which has recently had a malaria outbreak, Greece.
Very few cases/deaths compared to Italy -
Costa Rica has malaria so only 6 deaths so far. Highest malaria cases in the swampy east of the country with very few COVID 19 cases, again correlates well with taking ant-malaria meds. As in all other malaria infested regions worldwide.
-
Tonic water has reappeared on our supermarket shelves after a recent run on it (due to the presence of quinine 20 mg/litre). From the pharmacokinetics of HCQ paper therapeutic serum levels of 2mg/L are only achieved 2-3 days after giving even high initial doses of 800 mg/day. Part of this will be due to excretion by the kidneys, conversion to metabolites desethyl HCQ (also thought to be active) by the liver but also a large fraction would be due to the 1000-fold concentration into intracellular compartments. By taking a low prophylactic dose of quinine supplied by consuming a litre of tonic water per day there would be some saturation particularly of the intracellular concentration from nM serum levels to uM intracellular levels. Against such a background level, a high therapeutic serum level of HCQ on the appearance of COVID19 fever symptoms could occur much more rapidly, or even better with a low prophylactic dose of HCQ if available (malarial dose of 400 mg once a week then 400 mg per day on first fever symptoms). This long time lag before HCQ can reach therapeutic levels may well account for the poor results in some of the ICU studies particularly the veterans and the Brazilian papers, in which it is used at a late stage in the illness which would effectively be running its course untreated for 2-3 more days until plasma levels reach the therapeutic target of 2 mg/L after giving even a high dose (600 mg). There also appears to be a time lag in Raoult's results of 48 hours before any reduction in viral load occurs with his HCQ alone treatment, whilst the azithromycin probably has therapeutic effect reaching high plasma levels within an hour or so. Similarly for Zn in Zelenko's case. So carry on drinking tonic water (Gin too according to Eric Swartz's alcoholic ideas) - it used to work out in India!
-
Or in other words about this negative anecdotal veteran's study from comments:
It was not a randomized clinical trial in any sense of the word. It was a collection of anecdotes with some statistical manipulations used to try to reverse engineer some randomness into the cohort selections. It used a method called PSM for randomization and this method is no longer recommended for use as it can introduce bias. There are better ways. Zinc was never once mentioned in the study but zinc is a crucial element in the HCQ "cocktail". At the very least they should have randomized on patient zinc status. Zinc deficiency is extremely common among the elderly. Not even one doctor was interviewed to get a sense of what the decision criteria was for using or not using HCQ. This has a massive potential for introducing invisible bias into the results that PSM cannot remove. Dosages used are not discussed. And lastly, the HCQ was administered too late in the disease progression at the point where cytokine storm was the dominant factor determining outcome, not viral replication. In this case the Z-pack which combats the CS apparently showed some efficacy. A good study would have more patients and the treatment protocols need to be well defined. This study is actually much worse in that regard than the much criticized French study.
-
We will all eventually be infected so better to get it over with now rather than later - we just have to take the anti virals at the right time as in Mass Fever Treatment as recommended by the WHO for malaria. So allow the antibody response to occur then kill off the virus with our ANTI-Bat Combo. Just like vaccination without having to spend two years developing one.
-
Competing interests?
Competing Interest Statement
Disclosure forms provided by the authors are available with the NEJM. JA is a co-founder of iVeena Holdings, iVeena Delivery Systems and Inflammasome Therapeutics, and has received consultancy fees from Allergan, Biogen, Boehringer Ingelheim, Immunovant, Janssen, Olix Pharmaceuticals, Retinal Solutions, and Saksin LifeSciences, all unrelated to this work. JA is named as an inventor on a patent application filed by the University of Virginia relating to Covid-19 but unrelated to this work. SSS has received research grants from Boehringer Ingelheim, Gilead Sciences, Portola Pharmaceuticals, and United Therapeutics, all unrelated to this work. The other authors declare no competing interests.
.....and
Hydroxychloroquine has been reported to inhibit SARS-CoV-2 replication in vitro with a 50%
maximal effective concentration (EC50) ranging from 4.5 μM to 17 μM.17 However, the approved
dosing regimens for hydroxychloroquine in patients with rheumatoid arthritis or lupus generate
substantially lower peak serum drug concentrations (~1 μM).18,19 AConfusing because HCQ EC50 was 0.37 uM. CQ was 1.1 uM, Corresponding EC90's were as quoted HCQ 4.5 and CQ 17 uM. Then Lupus patients taking 400 mg HCQ daily would have a serum level of nearer 10 uM not 1 uM.
-
Check out the original paper and you'll find that one of the authors has links to Gilead who make remdesivir and others are linked to other Pharma companies. They've skewed the data to look a lot less promising, even quoting EC90 values for HCQ as being EC50's (anybody else spot the deliberate misquoting to make it look less effective in vitro?). I think Wyttenbach did. Let's face it they still want to make a killing out of their own patented big Pharma drugs and when a cheap remedy comes along vested interests dictate they squash the opposition. Another war going on against the cheaper favipiravir (Avigan) no doubt since it originated in Japan and was since mass produced in China. Fortunately for the Germans (and Indonesians) Merkel saw through the BS used her own scientific judgement and is now stockpiling Avigan & distributing to hospitals and universities using the military. Been using HCQ successfully too as are the French Spanish and Italians, all of which are showing improvements in daily death rates and reductions in active cases since 25 March - 2 April. But not the UK as a control. Then look at what happened to the Chinese stats showing dramatic recovery after Bayer shipped them a free load of CQ on Feb 20! It's not just the effect of lock down after the first publication of the Wang in vitro report on Feb 2 pharmacists the world over realized it's potential ! - resulting in an embargo in the UK (idiotic), Zelenko treating people in NY and Didier Raoult's flawed studies in France. How much more of a mess could idiotic humans make out of a very simple biochemical observation that CQ or HCQ blocks CV entry, replication etc. It works, forget the anti Trump and Macron BS propaganda built up around it. All because a guy in Arizona drank some fish tank cleaner or some poor two year old died of an overdose 37 yrs ago (very very sad but surely the parents should know not to leave drugs lying around like smarties)
And at long last another virologist has recognised the correlation between anti malarial drugs use and almost complete absence of COVID-19 cases, the correlation I posted here with detailed mapping etc. No other epidemiologists like Ferguson's group interested? Too preoccupied with mathematical modelling, promoting testing, shutting down the economy without even considering possible treatments. The Chinese have come out of their quarantine, their economy will thrive, downplaying all along their widespread mass distribution of CQ, HCQ and Avigan playing a role in their recovery. Quote 'HCQ no more effective than other normal therapy (ritonavir/lopinavir!). Politics both East and West!
-
Like in the Brazilian study, why wait until the patients are half-dead on ventilators before giving them anti-viral therapy. Generally in Europe and specifically Zelenko's trials involve treatment at a very early stage in the illness before significant disease pathology has occurred. More about that other scoundrel Didier Raoult, and
at last somebody else on the planet has made the correlation between anti-malarial drug use of mefloquine and chloroquine and very few numbers of COVID-19 cases and fatalities!QUEST FOR CHLOROQUINECoronavirus: Didier Raoult the African and chloroquine, from Dakar to Brazzaville
IN DEPTH This article is part of the dossier:Corona Chronicles: 13 April – 17 April
By Marième Soumaré, Rémy Darras
Born in Senegal, where he spent his childhood, the French doctor and researcher has maintained strong professional and emotional ties with the continent. And many African countries are already using chloroquine to treat people infected with Covid-19.
On 24 March, Professor Didier Raoult slammed the door on the circle of researchers who were supposed to advise the French president on the pandemic.
Disagreeing with the containment policy adopted by France, which favours mass screening, the iconoclastic infectiologist has just been disavowed by his peers, who are reluctant to endorse the use of hydroxychloroquine against coronavirus.
On Thursday 9 April, Raoult could measure the progress made when President Emmanuel Macron travelled especially to Marseilles to talk to him in order to “take stock of the question of treatment.”
This was a strong political gesture in favour of Raoult’s theses, whose promotion of the use of hydroxychloroquine to treat coronavirus patients has been the subject of much controversy for several weeks.
READ MORE: Coronavirus: 9 things to know about chloroquine
Pre-COVID-19 era
A specialist in emerging tropical infectious diseases at Marseille’s Faculty of Medical and Paramedical Sciences and at the Institut Hospitalo-Universitaire (IHU) Méditerranée Infection, the long-haired professor with the pepper and salt beard was still largely unknown to the general public at the end of February when his views on a chloroquine-based coronavirus treatment began to be heard.
Since then, the Frenchman has seen his media and digital fame take off. And in the ranks of its most fervent supporters, the African continent is not to be outdone.
Is it because the chemical compound he uses to treat his patients, hydroxychloroquine, is well known on the continent, where it has long been used to treat malaria? In two publications exposing tests carried out on some 20 patients, then on 80, the researcher and his teams conclude that “hydroxychloroquine combined with azithromycin is effective in the treatment of COVID-19”.
This quinine derivative is currently the subject of several studies. Those carried out by Professor Raoult have indeed aroused reservations among many experts, who reproach him for not having respected standard scientific protocols. At the end of March in France, the High Council of Public Health considered that chloroquine could be administered to patients suffering from “serious forms” of the coronavirus.”
READ MORE: To fight coronavirus, Burkina Faso is tempted by chloroquine
Those African countries that opt for chloroquine
At Fann Hospital in Dakar, Professor Moussa Seydi, head of the department of infectious and tropical diseases, has already administered chloroquine alone to the first 100 patients who tested positive for COVID-19. “In Marseille, Dr Didier Raoult published encouraging preliminary results. The combination of hydroxychloroquine and azithromycin should make it possible to shorten the carrying time [of the virus], in order to accelerate the healing of the sick,” Seydi told Jeune Afrique on 19 March. To use this drug, he says he relied on the study co-signed by his French counterpart.
Like Senegal, Burkina Faso, Algeria and Morocco have also opted for chloroquine.
On 23 March, the Ministry of Health of the Cherifian Kingdom thus requisitioned the national stocks and distributed to the directors of CHU the protocol for the prescription of chloroquine and hydroxychloroquine for confirmed cases of COVID-19. A decision inspired by Chinese research on the subject, and studies conducted by the French researcher, according to a member of the Moroccan committee in charge of the fight against the pandemic.
Born and raised in Senegal
If Professor Raoult is well known on the continent, it is also because this specialist in tropical and infectious diseases, in addition to having grown up there, has worked a lot there. It was in Dakar that the Frenchman is said to have caught the research virus.
Born in 1952 in the Senegalese capital, he lives there, in the building of the Research Office for Food and African Nutrition (Orana), created by his father.
This building sits opposite the Pasteur Institute in Dakar which houses the frontline laboratory in the fight against the epidemic in Senegal, and is where this son of a nurse and a military doctor stationed at the capital’s main hospital, took his first steps.
A childhood marked by happy memories of playing on the beach at Anse Bernard, made the move “complicated” when the young Didier Raoult arrived in Marseille at the age of 9. “Being partly Senegalese, I can’t help but feel concerned by what’s happening in Africa,” he says in a video addressed to the Senegalese group eMédia on 7 April.
Research on all fronts
Sokhna, also a Senegalese, is director of research at the Institut de recherche pour le développement (IRD), and regularly exchanges with Professor Raoult. This week, IHU’s Senegalese team of about thirty people was due to submit a research project to the Senegalese Ministry of Health on the protocol of the chloroquine-azithromycin combination.An encouraging sign, according to Sokhna, is that the prevalence of coronavirus seems to be lower in areas where the use of antimalarial drugs such as chloroquine or mefloquine is frequent.“This can be seen very crudely. But other factors will have to be taken into account before any definitive conclusions can be drawn,” adds the enthusiastic and cautious researcher, who is usually based in Marseille but is currently on a long-term mission in Dakar.This mixed research unit is far from being the only innovation driven by Didier Raoult in Africa. In 2012, the French researcher installed a MALDI-TOF at the main hospital in Dakar: a mass spectrometer that can detect bacteria in a few hours, compared to the usual two to three days with traditional methods.





